
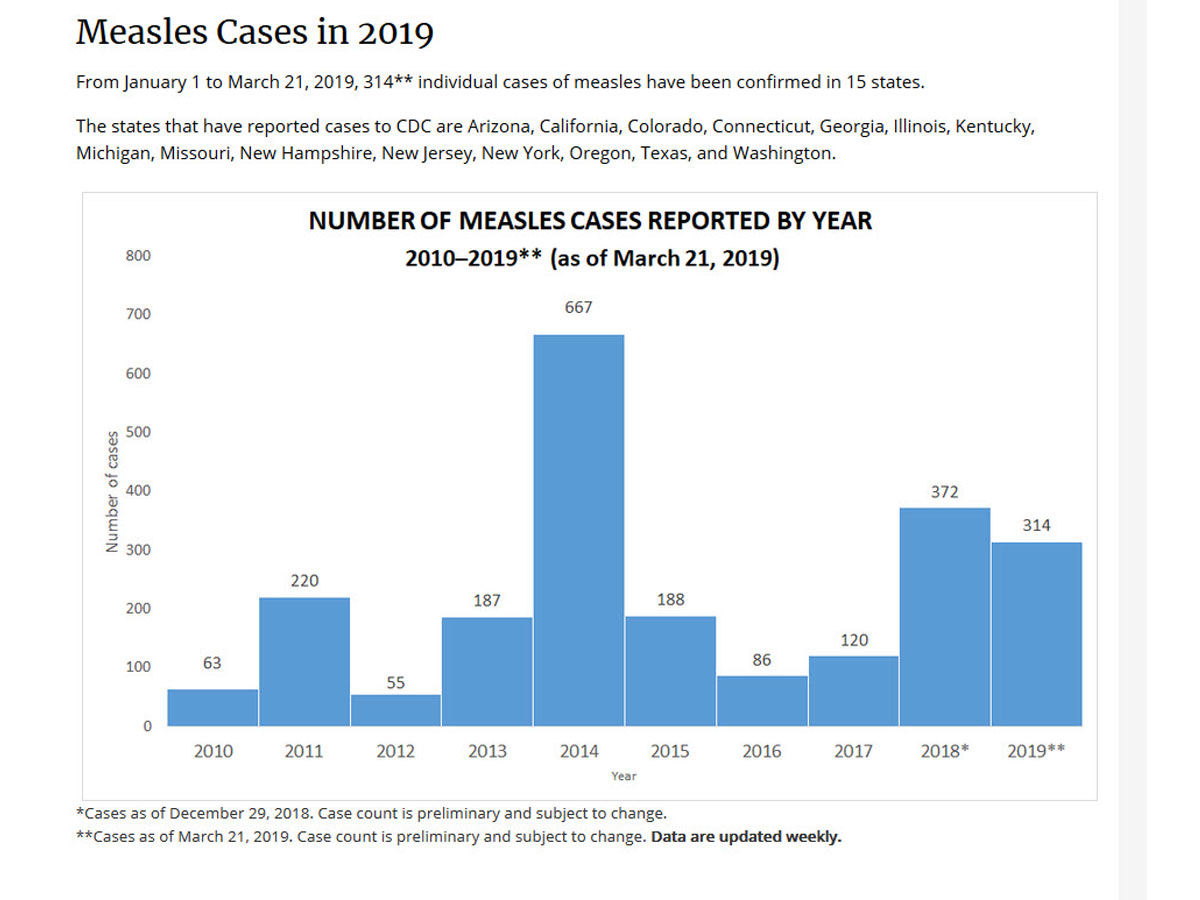
Vaccines have been a topic of conversation in my lectures lately, especially since the recent Measles outbreaks in the Pacific Northwest. Below is my own personal take on vaccines based on current scientific knowledge and practices.
Types of Vaccines
There are different types of vaccines. The first is called a “killed” or “inactivated” vaccine which includes the dTAP (tetanus, diphtheria, pertussis or whooping cough) , most versions of the flu shot, and polio vaccines. Killed vaccines have completely dead versions of the pathogens in question and as such do not require as much refrigeration or preservatives as the next type of vaccine. “Live” vaccines, which include the MMR and chickenpox vaccines, contain a weakened or partially killed form of the virus in question and require preservatives and refrigeration to be kept effective. Usually this preservative is neomycin, an antibiotic in the name brand Neosporin.
For more information on types of vaccines, check out these links:
https://medlineplus.gov/ency/
https://www.vaccines.gov/
Vaccine Risks
Like any drug, different vaccines carry different risks so you should always consult with a medical professional. The idea with killed vaccines is they confer immunity without the small risk of contracting the actual illness that exists with live vaccines. On the downside, the killed vaccines may have to be “boosted” more often whereas live vaccines are intended to confer lifelong immunity with one or two shots. Aside from the small risk of contracting the actual disease from a live vaccine there is also the chance of allergic reaction (either to the virus or the antibiotics/preservatives) or something called aseptic meningitis. This condition is a dangerous swelling of the brain that can, if untreated, lead to hearing loss and possible cognitive difficulties. That being said there are different strains of the vaccines that carry a higher risk. In addition, meningitis also occurs in about 20% of the people who contract the mumps virus so if you are unvaccinated and exposed to mumps you can still get damaging encephalitis and other life-threatening symptoms.
Strains of Mumps Used in Vaccines
In 1988 the UK and some other European countries introduced a MMR vaccine where the mumps component was isolated from the Urabe strain and marketed under the name Pluserix. This vaccine carried a higher risk of contracting meningitis but conferred a higher efficiency in terms of preventing the contraction of the mumps virus. Due to several cases in the UK and elsewhere of aseptic meningitis correlated with the Urabe strain, it was discontinued in several countries in the 1990s and today only exists in the developing world where efficacy at preventing mumps and mumps-related meningitis may outweigh the risk of aseptic meningitis from the vaccine itself. In the US, a Jeryl Lynn strain was developed int the 1970s, named after the daughter of the vaccine creator who took the strain samples from his sick daughter Jeryl. This strain of the vaccine is more expensive to make, which is perhaps why some countries have done away with vaccinating against mumps at all, like Japan where a Measles-Rubella vaccine is in use.
For more information on the strains of MMR vaccines, check out these links:
The RIT 4385 strainis derived from the Jeryl Lynn strain by Maurice Hilleman (Jerly Lynn’s father). (Hviid A, Rubin S, Mühlemann K (March 2008). “Mumps”. Lancet. 371 (9616): 932–44. doi:10.1016/S0140-6736(08)60419-5. PMID 18342688)
The Leningrad-3 strainwas developed by Smrodintsev and Klyachko in guine pig kidney cell culture and has been used since 1950 in former Soviet countries. (“Immunizations, Vaccines and Biologicals – The Mumps Vaccine”. World Health Organization. Archived from the original on 2006-04-23). This vaccine is routinely used in Russia.
The L-Zagreb strainis used in Croatia and India and derived from the Leningrad-3 strain by further passaging. (“Immunizations, Vaccines and Biologicals – The Mumps Vaccine”. World Health Organization. Archived from the original on 2006-04-23).
The Urabe strainwas introduced in Japan and later licensed in Belgium, France, and Italy. It has been associated with a higher incidence of meningitis (1/143,000 versus 1/227,000 for J-L). ( “MMR Vaccine”. Pediatric Oncall. January 7, 2006. Archived from the original on April 30, 2007.) It has been abandoned in several countries and was formulated as MMR in the UK.
The Rubini strainwas used mainly in Switzerland and was attenuated with a higher number of passes through chicken embryos. It later proved to have low potency. (Eurosurveillance report on Portugal outbreak. Archived September 7, 2005, at the Wayback Machine). It was introduced in 1985. (“Immunizations, Vaccines and Biologicals – The Mumps Vaccine”. World Health Organization. Archived from the original on 2006-04-23.)
The Autism Claim
Andrew Wakefield, the author of the first paper that claimed a link between autism and vaccinations, based his paper on 12 children and drew a link between the MMR vaccine given at 12-15 months and the development of Crohn’s disease and inflammatory bowel disease (IBS). His argument was that this inflammatory disease then lead to neurological symptoms. (https://www.nytimes.com/2011/
Errors in Wakefield’s position:
- Conflict of Interest.Wakefield received financing from private lawyers preparing to sue the vaccine manufacturers before he published his paper. He failed to disclose this and other conflicts of interest to the journal and his co-authors who later asked for their names to be removed from the paper. The Lancet journal later fully retracted the paper in 2010.
- Flawed Precedent.Wakefield’s argument would mean any children with Autism caused by MMR vaccines would also have preceding cases of Crohn’s disease or IBS. Many of the later claimants’ children did not follow this pattern.
- Falsified Data.A medical board hearing in the UK where this all took place stripped Wakefield of his medical license after finding that he fudged the onset of IBS and autism symptoms to appear closer to the date of vaccination than actually occurred.
- No Identified Vaccine.I could not find anywhere in the original article or follow up reviews which type of vaccine the children actually received. Was it the Measles Rubella? The Measles mumps rubella? The Urabe strain or the Jeryl Lynn strain? For the time period this controversy covered (1988 to present) there have been more than 10 different types of vaccines relating to these viruses developed.
- Wakefield Wavers.Wakefield still stands by his claim that he believes the MMR vaccine may lead to autism, however in 1998 he explicitly stated “Do vaccines lead to autism, I don’t know. I am not anti-vaccine I am safety first and the current vaccine schedule in this country (UK) is not safe”. This statement makes it appear he has wavered from his own claim of the link between MMR vaccines and autism.
For more information on Wakefield’s claims, check out these links:
https://www.thelancet.com/
WHO Vaccine Schedules
The World Health Organization has a list of the current mumps vaccine types available, including the requirements and recommendations for vaccine schedules of different countries, https://www.who.int/
Before Getting a Vaccine
When considering a vaccine, perform the following safety checks.
- Get information from more than one source. Your doctor/nurse/nurse practitioner may claim it is perfectly safe, but that could be what they were told.
- Compare the possible side effects of the vaccine with the dangers of contracting the targeted illness.Is the disease worse than the vaccine? Or are the side effects of the vaccine and the possible future health implications worse than the actual disease?
- Consider your encounter risk.How often are you exposed to people, especially children, who may have this illness? Do you have vulnerable family members (infants, cancer patients, elderly, disabled) who could catch the disease from you?
- Does the pharmaceutical company who makes this vaccine have a history of making dangerous vaccines?Do pharmaceutical companies lie to protect their interests? Of course they do, https://en.wikipedia.
org/wiki/List_of_largest_ pharmaceutical_settlements. If the vaccine manufacturer’s name is on this list, you should probably look for a different vaccine or maybe reconsider whether you need one.
Vaccinations and World Health
Although not all vaccines are created equal, the MMR vaccines have been successful in reducing measles, mumps, and rubella related deaths in children all over the world, https://www.historyofvaccines.
So what did you learn from this information? Are all vaccines created equal? NO. BUT speaking with a medical professional and weighing the pros and cons of your particular situation are important for protecting yourself and the ones you love.
I hope this information had been helpful. As always, if you have questions, you can ask me after class.
